IHO’s HISTORY…
|
|||||
|
To start with, IHO donors in the United States and India provided the initial seed money, resources and technology for the program. Then IHO formed a group of volunteers made up of South Asian expatriates, U.S. citizens, local experts and NGOs to work with the people living in rural communities in Bihar. These volunteers trained some of the women of the community as health educators who then went out and trained others in health and proper hygiene techniques. This enabled the women from the local community to prevent the contamination of their water source and maintain a healthy living environment. We call this our “self-help” model for community development. Our rural health model comprised of providing hand pumps for water and sanitation, health education through women educators, and thence adding mother-and-child health programs. Our self-help model provides ongoing education and support in a way that is cost-effective and perfectly suited to the local culture and environment. |
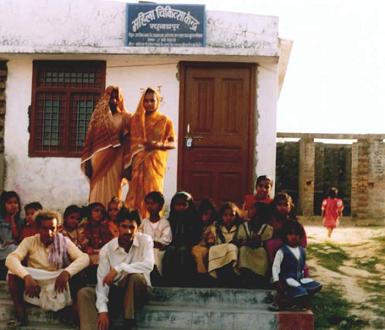
Group outside IHO’s health center in Bihar |
||||
|
In summary: The underlying theme of IHO programs is that improved environmental health is the most basic need of rural, underdeveloped communities and that its two components – community health and community development – are interdependent and need to be focused upon concurrently and equally. We have proven over the last 25 years that our integrated and holistic health program that combines clean water and sanitation facilities with health, hygiene and vocational training is transferable to rural communities in many developing countries. Details of our initial findings have been presented and discussed at several national and international meetings, including several annual conferences of the American Public Health Association (APHA) in the United States and the World Federation of Public Health Associations (WFPHA) in Indonesia since 1992 itself! Current status & future goals: IHO currently runs its programs in more than six states in India, Nepal, Bangladesh, Bhutan, Sri Lanka and other developing countries in Asia and Africa. By 2025, we aim to implement our program in most of the developing countries. Our goal is keep our programs self-sustaining aided by a large pool of volunteers. |
|||||
